The Small Barrel, like the Spine Corrector and the Ladder (Large) Barrel, is distinctive for its curved shape (Figure 1). This allows for many advantages in the Pilates Contrology method of body conditioning. One that we would like to point out here is working with the rounded curves of the spine, specifically thoracic hyperkyphosis.

Figure 1. Small Barrel. Permission Simona Cipriani (www.artofcontrol.com).
The healthy spines should have curves that are described as kyphotic and lordotic (kyphosis and lordosis). The thoracic (mid-back) and sacral (pelvic) spines should be kyphotic, and the lumbar (low back) and cervical (neck) curves should be lordotic (Figure 2).
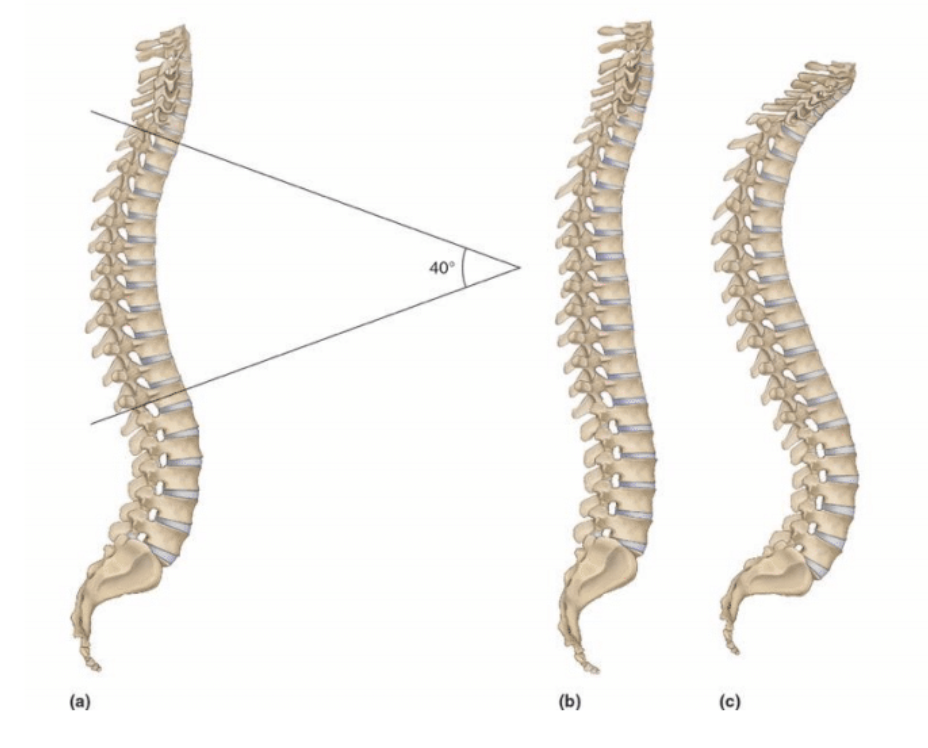
Figure 2. Right lateral views of the spine. In Figure 2a, we see a healthy thoracic kyphotic curve of 40 degrees. Figure 2b shows a hypolordotic thoracic curve. Figure 2c shows a hyperkyphoticthoracic spine. Permission Dr. Joe Muscolino (www.learnmuscles.com). Artwork by Giovanni Rimasti.
However, postural distortion patterns can occur in which one or more of these curves can be increased (e.g., hyperkyphosis, hyperlordosis) or decreased (hypokyphosis, hypolordosis). One of the major aims of Contrology is to help the client who has a postural distortion pattern return to symmetry and/or healthy posture. Given that we are speaking about spinal curves, it makes sense that working with a curved surface like the small barrel would be ideal toward working with these clients. Perhaps the most common postural distortion pattern in the human body is hyperkyphosis of the thoracic spine, which involves excessive thoracic flexion, and is also known in lay terms as rounded back. This pattern is fast becoming the most common distortion pattern due to the increased use of digital devices, especially the smart phone and tablet (Figure 3).
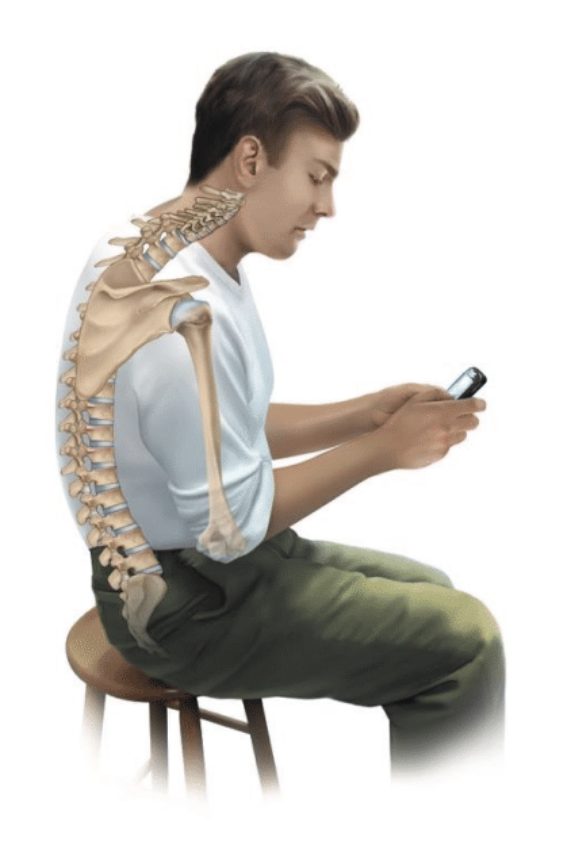
Figure 3. Hyperkyphosis of the thoracic spine. Permission Dr. Joe Muscolino (www.learnmuscles.com). Artwork by Giovanni Rimasti.
Any habit pattern that asks us to flex our spine forward in flexion to work down in front of ourselves can lead to thoracic hyperkyphosis. It should be pointed out that reading books and working with pen and paper similarly involves flexion of the thoracic spine, but the ever-increasing number of hours spent with digital phones and tablets is the primary factor causing the tremendous increase in the number of clients presenting with thoracic hyperkyphosis. There is an old saying: There is no such thing as a bad posture, as long as you don’t get stuck init. The problem is that if we spend large amounts of time in thoracic hyperkyphosis (or any posture for that matter), we will get stuck in it. Getting stuck involves neural facilitation patterns of muscle contraction, called muscle memory in lay terms. This involves some muscles being acilitated and tightening up(locked short)at baseline tone, and others being inhibited and weakened (locked long)at baseline tone.It also involves fascial adhesions that, as the term describes, adhese/glue the tissues together by the accumulation of fibrous fascial collagen tissue; paramount among these tissues are the ligaments and joint capsules of the spine. The sum total of all this is that the spine gets stuck in flexion and loses its ability/flexibility to move into extension.
Let’s explore how the small barrel can help our clients with thoracic hyperkyphosis. Given that thoracic hyperkyphosis is an excessive flexion of the thoracic spine, our goal is to introduce force of extension. The key to the small barrel is the rounded shape. A flat surface, such as the Mat, Cadillac, or carriage of the Reformer, cannot effectively place an extension force into the thoracic spine. But a rounded convex-shaped piece of apparatus can. If we have the client lie supine on the small barrel with the apex of barrel’s curve under the thoracic spine, then the weight of the client’s body will cause the spine above and below the barrel’s apex to fall around it into extension, thereby mobilizing the thoracic spine into extension at that vertebral joint level (Figure 4).

Figure 4. A person lying supine on a gym ball demonstrates how their body falls around the apex of the ball. Permission Dr. Joe Muscolino. Artwork by Giovanni Rimasti.
This is an effective means of focusing the extension force to the desired spinal level. The barrel can then be moved to have its apex at another spinal joint level (Figure 5).

Figure 5. A person lying supine with the Small Barrel under their upper thoracic spine. Permission Simona Cipriani (www.artofcontrol.com).
Doing this throughout the thoracic spine, or at least throughout the spinal levels that are most adhesed into flexion, can be an extremely effective means of lessening the client’s thoracic hyperflexion. Muscles and fascial tissues (ligaments and joint capsules) that are locked short will be stretched out, not only decreasing the hyperflexion of the thoracic spine, but also increasing the extension range of motion/flexibility. The beauty of this type of work with the Small Barrel is that it simulates manual therapy (GradeIV, slow-force) joint mobilization of the spine into extension by focusing the extension mobilization at specific spinal levels, perhaps obviating the need for the client to see a manual therapy physician or manual therapist (e.g., chiropractic or osteopathic physician, or physical or massage therapist).
___________________________
Precautions
Of course, there are certain cautions that should be observed. The first is that any force applied to the client’s body must be done carefully, slowly, and incrementally. Asking for too much of a change too quickly can cause harm, by either literally damaging the structural integrity of tissue, or by causing the nervous system to hyper-vigilantly respond with protective muscle spasms. It might be best to begin with the apex of the small barrel away from the most restrictive area of the client’s spine (which is usually the apex of their thoracic hyperkyphosis), and gradually over many sessions(weeks or perhaps many months)work toward the apex of their curve. Another note of caution is that if the client is elderly and has been in hyperkyphosis for many decades, it is possible that they have developed cervical (osteoarthrotic) fusion of the thoracic vertebrae. If this is the case, it is no longer possible to introduce extension (or any) motion into their thoracic spine; and attempting to do so will only aggravate their back. And one other caution is if the client has osteoporosis, in which case any direct force into bones, vertebrae in this case, is precautioned against, or perhaps contraindicated. However, having clients with these precautions are rare, and for the vast majority of our clients, using the small barrel to help remedy hyperkyphosis is extremely beneficial.